

An Algorithm for Nurses
As a longtime healthcare provider, Frank Aviles Jr., PT, CWS, FACCWS, CLT, would like to believe that most wound care patients have the benefit of being treated by clinicians who are informed on best practices per evidence-based medicine (EBM). But the truth is that he can’t confidently say that this is the expectation — at least not to the degree that the late David L. Sackett, MD, et al described it as in the late 1990s.1
“Dr. Sackett defined evidence-based practice as the judicious use of clinical expertise and skills with the integration of relevant clinical research with education, and due to multiple constraints it is difficult for clinicians to expand their skills and education while keeping up with pertinent research,” said Aviles, the wound care service line director at Natchitoches (LA) Regional Medical Center. His comments are not meant to slight anyone. As one who works in a rural setting, Aviles knows well that the challenges he refers to are not easily avoidable. He and his colleagues must coordinate the opportunities that they have to receive continuing education because allocating staff members to cover for those providers who are not on the floor on a given day, even if their absence is due to the pursuit of education, requires a commitment from all involved. A certified wound specialist who also moonlights as an educator, teaching various courses across the country on lymphedema management and other comorbidities that affect wound care patients, Aviles says that he wants to be part of the solution – as opposed to simply acknowledging the problem. He recently developed an algorithm to assist nurses and other healthcare providers when considering the course of treatment for diabetic foot ulcers (DFUs), which are considered to be “the most common occurring problem” in the world.2
Aviles recently spoke with ADVANCE to discuss his inspiration for the algorithm, how it functions, and how nurses can utilize it as members of the healthcare team and to advocate for the well-being of their wound care patients.
Algorithm & Education Needs
The biggest issue as it relates to providing optimal wound care to today’s patients is that there are not enough clinicians who are properly educated on the treatment of chronic wounds. “Properly educated” is the key takeaway here, and the problem begins at the foundational level, according to Aviles. “Wound care education is typically limited beginning at the academic level,” he said. Another dilemma is that primary physicians may still be trying to care for chronic wounds in their office setting as opposed to referring their patients to an outpatient clinic. Although this trend does not appear to be as pervasive as in years past, as wound clinics and other clinical settings become more accustomed to collaborating with referred patients through accountable care organizations, as an example, there still may be a tendency for primary physicians to not refer patients to specialty clinics as quickly as they should. This may put wound care nurses and other clinicians in the outpatient setting at a disadvantage and may lead to hospitalizations where very sick patients present challenging cases that may have been avoided had a referral been made early on.
“When primary providers have patients who are diagnosed with cancer, they are going to refer them to an oncologist immediately — they do not try to manage these patients themselves for an extend time before they make the referral like they often do with wound care patients,” Aviles explains. “But wounded patients will have better outcomes if they get referred initially to a wound specialist.”
The idea for the decision-making algorithm piqued Aviles’ interest many years ago, when more students he came into contact with through his classes began to follow up with him to ask about proper treatment and other advice despite their being staffed at specialty clinics. As clinicians continued to reach out to him he became more anxious to perfect it, finish it, and share it. “The consistent message is that some healthcare providers may need guidance in looking at the diabetic patient comprehensively when caring for their wounds,” he said.
“We understand that acute wounds heal in an expected time frame as they progress through the overlapping cascade of events. But chronic wounds may linger, and increased tissue damage with the passing of time may result in amputation. When consider other comorbid conditions, wound management becomes even more difficult. Today’s clinicians need guidance on not just knowing what’s ‘right’ for their patients but also knowing what is right. What once began as a ‘cheat sheet’ guidance for clinicians to care for DFUs grew into a tool that helps clinicians to assess the wound and the patient, and then consider several aspects of their care that will impact the progression of healing for these chronic wounds based on their findings.”
Algorithm Components
All clinicians will understand the challenges that patients who have been diagnosed with diabetes also develop an ulceration, such as delayed healing, inability or delayed body responses to recognize an infection, decreased oxygenation, difficulty maintaining an acceptable glucose level, neuropathy, and gait abnormalities,” Aviles said. “But this algorithm is not to serve as a protocol or actual treatment regimen for DFUs. Instead, this tool can be used as a checklist every time a wound care patient is seen to ensure consistency in care and timely interventions.”
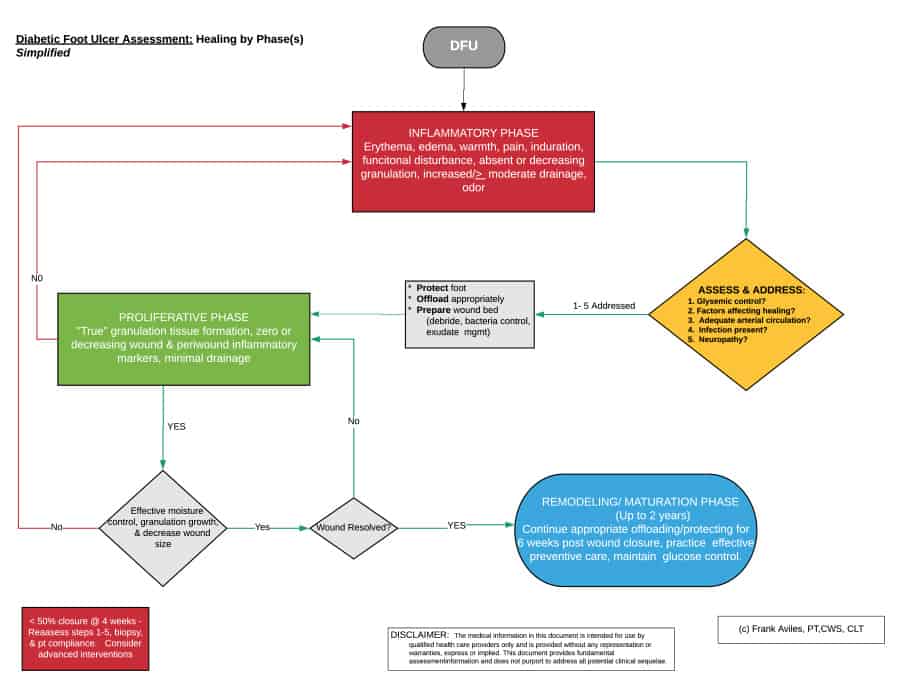
Designed as a three-phase process with individual steps noted within each phase, the material is presented as a flowchart that suggests a path of best practices as a way to help providers decide “what is right” based on the patient’s history and current wound status (phase of healing). Viewable on one page (see Figure 1), it’s meant to “help clinicians learn to do what is right in order to know what is right,” as Aviles explains, through the inflammatory, proliferative, and maturation phases. “At first glance it may appear overwhelming, but the intent is to offer a quick reference that can be consulted in the presence of the patient and/or other clinicians.” The algorithm is also available in what Aviles refers to as “a simplified version” (see Figure 2). Step 1 (of Phase 1) begins by determining if the patient has control of his or her glucose levels over an extended period of time. If these are not within acceptable ranges, the patient should be referred to their primary provider to improve glucose control, and Step 2 is then initiated while this treatment is ongoing. Step 2 calls for an assessment of factors and barriers that are directly affecting healing progression. Step 3 requires a screening of the patient’s large and small arterial vessels, which may lead to appropriate referrals and interventions. If abnormal or noted clinical signs of arterial insufficiency are found, the patient will require a vascular referral, the urgency of which will be based on test results. Step 4 is an assessment for local and/or systemic infection, and if an infection is noted, a culture will lead to proper antibiotics. Step 5 is an assessment of sensation. If neuropathy is present and/or a loss of protective sensation is determined, biomechanical assessment is recommended.
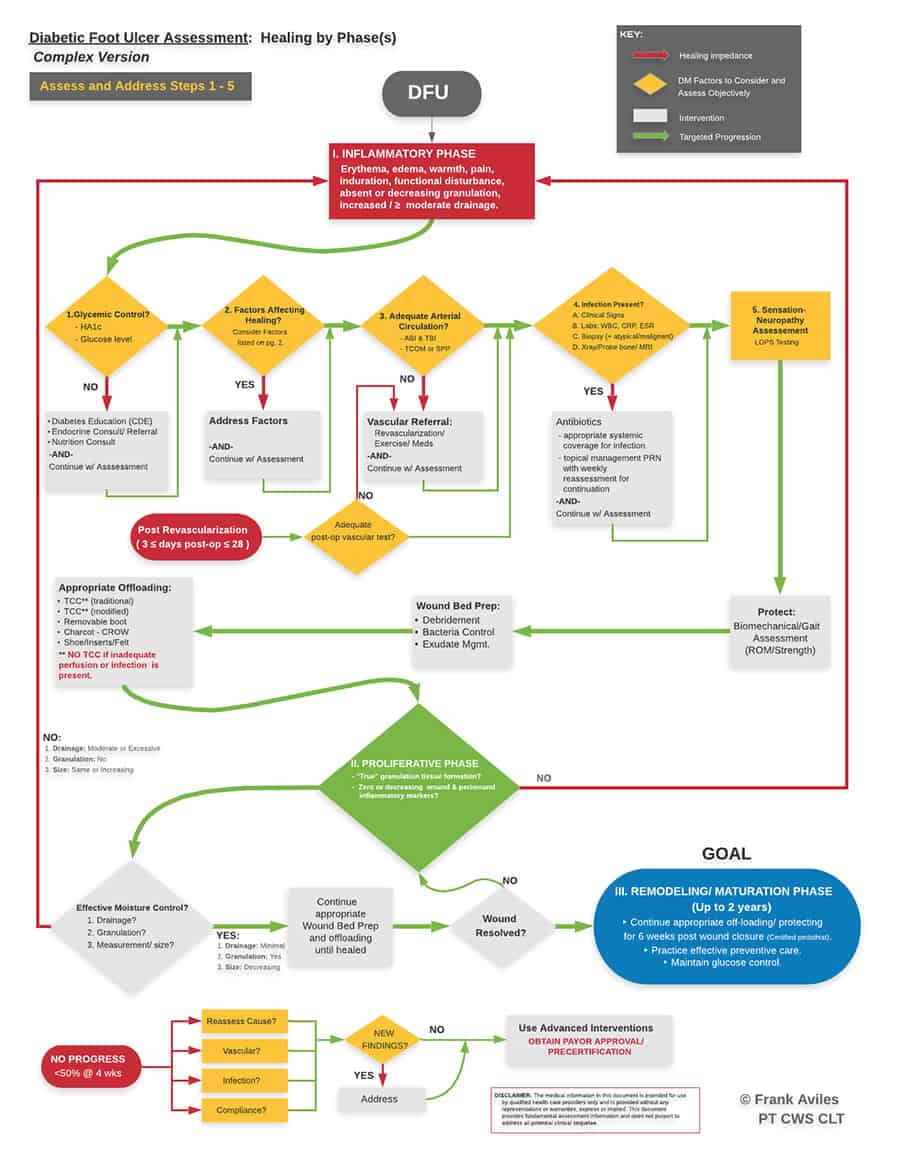
“Steps one through five will help determine how to proceed with interventions,” Aviles said. “At this point the wound should be improving to the proliferative phase and should now have granulation tissue formation with decreasing inflammatory markers and measurements. Drainage should also be decreasing also. If not, then the algorithm should be restarted until the clinician can answer “why” the wound is not progressing. If limited progress is noted, the clinician should carefully re-evaluate the cause, vascular status, potential infection, and the patient’s adherence to care management. At this point the considerations of advanced interventions may be required.”
Phase 2 asks the clinician to observe drainage, granulation, and wound size while continuing appropriate wound bed preparation and offloading until wound closure. During Phase 3, preventive care and glucose control are prioritized.
“As you review this document, keep in mind that the main focus is to determine interventions based on which phase of healing the wound is currently in,” Aviles explained. “The objective is to return all chronic, inflamed wounds to the proliferative phase, and there will be significant characteristics to identify when you have arrived at this phase. One common problem is that we utilize improper interventions at the wrong times because the wound is either in the inflammatory phase or keeps returning to it, and this problem usually means there are issues being overlooked or not addressed properly. When you begin at the top of the chart and see where you land based on wound presentation, there are lessons to be learned.”
Note To Nurses
Wound care nurses in particular can make an impact on EBM and improve patient outcomes, Aviles said. Specifically to nurses, what do you see as the benefits to learn and following this algorithm?Nurses are a critical member of any wound care team whether they are a rookie or a seasoned veteran in this field. In the nurse profession there are different types of nursing degrees along with differentbackgrounds. Wound care education is typically limited beginning at the academic level. There are manyassociations and certifications available with different focus making further education selection achallenge. This algorithm gives a one-page synopsis for nurses to refer to as they follow a few key steps to considerwhen treating a patient with a diabetic wound based on characteristics of the phases of healing. The aim is to refer the patients promptly if needed and begin aggressive interventions based on which phase thewound may be in.The number of wounds that do not progress through the phases of healing otherwise known as chronicwounds continue to increase in the United States. It has been said that there are 65 million people in the US suffering from these chronic wounds. These wounds consist of venous, pressure, and neuropathicwounds. Improving care and appropriate referrals for patients suffering from chronic wounds will lead toimprove outcomes and decrease mortality rates.
“Nurses are critical members of any wound care team, and improving care for patients suffering from chronic wounds will lead to improved outcomes while decreasing mortality rates,” he continued. Aviles also urges nurses to take the time to educate patients on their individualized treatment plan and to review he patient’s plan of care at regular intervals as a team whether or not the wound is making progress. “Keep asking ‘why’ when progress is halted or something does not make sense,” he said. “Be a patient advocate, and be consistent in not only doing what is right but knowing what right is. This algorithm is just another available tool that a healthcare team can decide to follow if together they deem it beneficial after reviewing the literature on best practices.
References
- Sackett DL, Rosenberg WMC, Gray JAM, Haynes RB, Richardson WS. Evidence based medicine: what it is and what it isn’t. BMJ. 1996;312:71.
- Raghav A, Khan ZA, Mishra BK. Financial burden of diabetic foot ulcers to the world: a progressive topic to discuss always. Ther Adv Endocrinology Metab. 2018;9(1):29-31.





